The Ultimate TRT Guide for Aussies – Part 4
The Ultimate TRT Guide for Aussies – Part 4
Let’s get right into where we left off from Part 3 where you can find here (Part 3 here). Why in Australia, despite the overwhelming evidence that testosterone enanthate should be administered 1-2 x weekly, do Doctors still prescribe testosterone enanthate every 10-14 days, which produces peaks and valleys that can bring about unwanted symptoms—and potentially harmful effects on the patient? There are a number of reasons, but the main reason is once again—the current prescribing guidelines in Australia that need an update. The below table is an extract from Endocrine Society of Australia and this publication is dated in the year 2016.
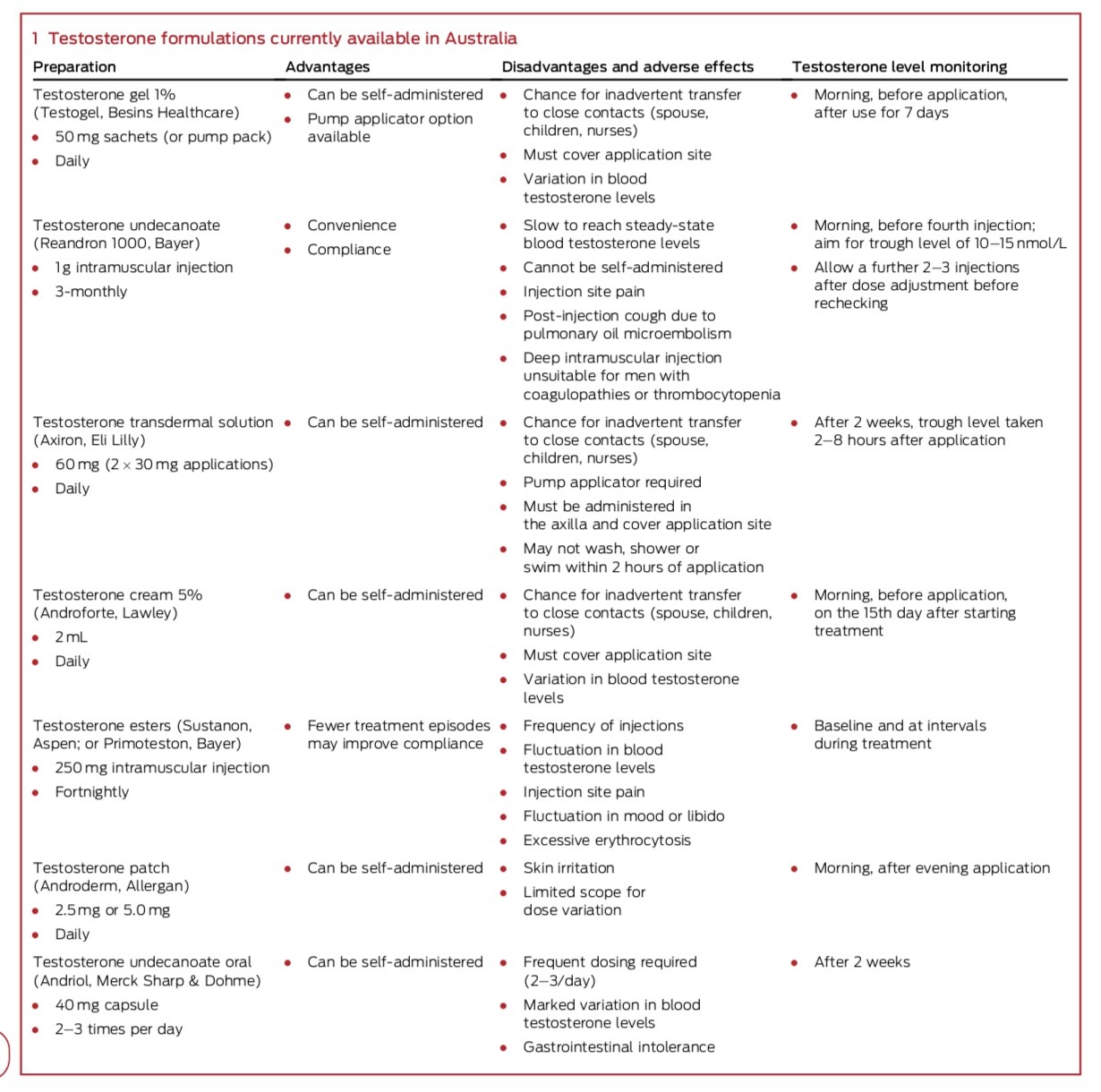
As you can read from the table, the guidelines state that testosterone enanthate be administered as 250 mg every 14 days intra-muscularly. The adverse reactions we discussed in Part 3 are also listed and all of these adverse events can be mitigated by splitting up the dose of 250 mg into 1-2 shots weekly, instead of once fortnightly. There is an argument a physician makes that the patient only receives an injection once a fortnight because it makes compliance easier. What does this mean? Simply put, according to medical professionals, it is apparently extremely inconvenient and often painful for a patient to have to receive an injection of testosterone and therefore, a once a fortnight injection makes for a more convenient administration schedule for the patient. You may be thinking:
“So let me get this straight. Despite the known fact that dosing testosterone enanthate once every 10-14 days will cause fluctuations in testosterone and estrogen which can cause unwanted symptoms, the every 10-14 days administration still stands as the recommended schedule all because the patient may endure a little inconvenience when it comes to injection time.”
I know right? It does not exactly weigh up in my mind either. Especially since sub-cutaneous (or shallow IM injections) have been proven in several study papers to be a safe an effective alternative to deep intra-muscular injection. Have you ever seen the needle provided with the Primoteston Depot (testosterone enanthate) prescription? It is not really a needle—more of a harpoon. Whether you choose intra-muscular, shallow intra-muscular or sub-cutaneous injection, all will be effective and should be easily administered by the patient, pain free. My recommendations are:
Intra-muscular injection: 1 ml syringe, 25-27 gauge x 1 inch needle.
Sub-cutaneous injection: 1 ml syringe, 27 gauge x ½ inch needle.
If asked what my personal favourite is, it is sub-cutaneous because of the painless and minimally tissue invasive administration. Almost all of the issues reported with sub-cutaneous injections I am sure I can resolve with a written Q & A so if you are experiencing any issues with sub-cutaneous injections, please do not hesitate in the comments section below. It is all in the method and technique. Once you have it, you will wonder how you ever survived with the intra-muscular way of life for your testosterone therapy. I put shallow intra-muscular in the same “convenience category” as sub-cutaneous and a lot of what people think is sub-cutaneous is likely shallow intra-muscular anyway. Absolutely though, gone are the days of using a 1.5 inch spear into your backside—that is as frightening as it is painful. I know Bayer will not pay much attention for some time, but I advise them to change their 250 mg/ml pre-filled 1 ml syringe that is accompanied with a javelin to use as a needle for injection. It just is not necessary. Science has evolved, and so the products and prescribing methods need to also. Unfortunately, if you are considering a blast in between your TRT, I do not advise sub-cutaneous injections if you want to put in large volumes of oil. I recommend no more than 0.5 ml (125 mg) at any one time/site via the sub-cutaneous method (and preferably less than that also).
While we have the table above us, I will briefly discuss the alternative methods offered for testosterone therapy in Australia.
Testosterone undecanoate 1000 mg single injection: A failed medication that requires a single, 4 ml injection every 3 months that is known to cause site pain and conflictions with injections for obvious reasons. This form of TRT will also cause fluctuations in testosterone and estrogen levels with the caveat that re-adjusting may take a much longer time than it would with enanthate because of the long half-life of the medication. I cannot see how this medication would be a good idea in any scenario unless you’re preparing for a short sentence somewhere that would make testosterone administration impossible.
Testosterone patches, creams and transdermal solutions: For some people these topical methods are preference and although I have a harder time fine tuning the tougher cases with topicals, if they are applied right, they do a good job at replacing healthy levels of testosterone for a patient. If a patient is considering the topical route, they need to pay extra attention with physically engaging with other humans/objects around the administration site, swimming, excessive sweating or anything that may potentially conflict with absorption. This disadvantage alone is enough to deter me away from the topical routes of TRT. The other caveat as I mentioned is that I often have a harder time achieving the right testosterone, estrogen, SHBG and DHT balance with the tougher cases when it comes to the topical routes. There is a narrower window for the physician to work with. All in all though, they work and can be the preferred choice for some over testosterone injections.
Sustanon 250 mg/ml: Sustanon works for some in the same way it does with testosterone enanthate, although I prefer to stay away from Sustanon because of the difficulty knowing what is causing what when symptoms arise. Sustanon is a blend of 4 different testosterone esters. Too many variables for my liking, but it can work well for some. Another mention worth noting is that it is not uncommon for some people to react negatively to testosterone propionate around the site and testosterone propionate is one of the esters contained within the Sustanon formula.
Testosterone Undecanoate Oral: Overall, taking testosterone with a glass of water actually can work; but one needs to be mindful that many will require multiple dosing’s per day (2-3 x daily) and so this may end up becoming a more expensive and inconvenient prescription than it first sounds. Also, as with almost any oral medication, there are often gastrointestinal side effects noted with those prone to GI issues. For those with a serious phobia with needles though, oral testosterone therapy can work, sort of.
All to be continued in Part 5. Until then everyone!
Add Comment